
One of the interesting tidbits gleaned from a presentation last week on the Medicaid expansion debate was that with expansion perhaps 60,000 Virginians now enrolled in Affordable Care Act Public Exchange plans will qualify for and switch over to Medicaid.
People who have low-enough incomes to qualify for Medicaid are also eligible for subsidies for an ACA exchange plan, so both programs are costing the taxpayers. A recent report indicated Medicaid is actually costing taxpayers less than ACA plans for that population.
UnitedHealthcare Group’s report noted – not a surprise – that Public Exchange coverage has proven to be more costly and less sustainable than envisioned (or promised). Since 2014 – the first year of Public Exchange coverage – the average annual unsubsidized premium for a benchmark silver plan has increased 88 percent for a 27-year-old and 76 percent for a 40-year-old.
The original projection was that it would reach 25 million persons by now, and in 2017 it was more like 10 million. Recent actions at the federal level will keep that from rising much beyond 12 million.
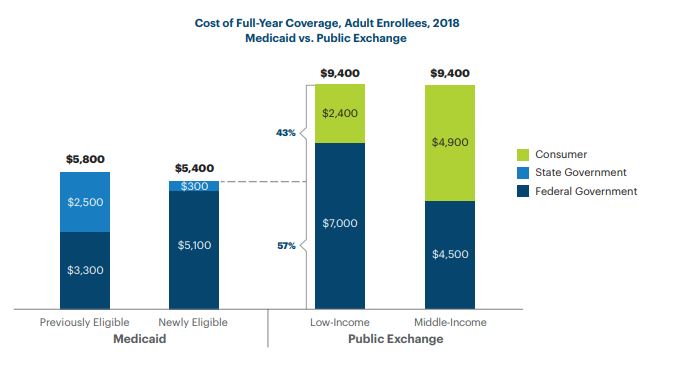
Compare that to Medicaid, which has enrolled more than 16 million additional people nationally since 2013. These figures are national, and Virginia would vary somewhat, but the estimated average cost for the newly eligible Medicaid enrollee has been $5,400 and the average total cost for Public Exchange coverage has been $9,400. In the case of the Exchanges, of course, much of that is coming from the consumer’s pocket.
But the low-income Exchange adult enrollees – the persons who could switch with Medicaid expansion – pay only $2,400 out of pocket and their federal share is about $7,000. That is still higher than the cost of Medicaid, which is fully government funded (state and federal combined).
This may not matter much to the Virginia voters and legislators opposed to expansion. The state taxpayer makes zero financial contribution to the ACA health plan subsidies, and is going to be paying a share of the cost for new Medicaid enrollees. We should find out early this week if the state Senate has a consensus on the expansion issue.
UnitedHealthcare Group (UHG) is hardly a disinterested observer in this discussion. It provides managed care for Medicaid in various states, now including Virginia, and based on its website it participates in some ACA marketplaces. If the company has an economic incentive to prefer one approach over the other, it is unlikely to admit that in these presentations.
But it does argue the billions planned for ACA subsidies would be better spent on Medicaid. It is unsaid but true that the future of the ACA Public Exchanges is cloudy at best, while Medicaid isn’t going anywhere, with or without expansion.
Absent from this is any discussion of quality outcomes when comparing the ACA Public Exchange plans with Medicaid, although UHG does advocate for managed care in general as providing higher quality for lower cost. And the cost of Medicaid is hardly expected to remain stagnant. Also absent is any discussion of which is preferred by the providers getting paid under the two approaches.
A footnote in the UHG report takes you to the most recent (2016) actuarial report on Medicaid. It was projecting federal costs would grow almost 6 percent per year, but also reported that the costs for newly-eligible adults were dipping slightly and might dip below those already eligible. As always the most expensive Medicaid populations were the aged ($14,323 per enrollee in 2015) and disabled ($19,478).
The audit noted most states that had opted for expansion were using managed care contracts to lower the costs. That will be the case in Virginia, and the 2017 Annual Report on Medallion 3.0, Virginia’s managed care approach, gives you a good idea of the services available. If this is a choice open to them the lower-income ACA covered population will probably make the change. It seems a very easy economic choice for them.
(Hat tip: Doug Gray)
Leave a Reply
You must be logged in to post a comment.