
 by Carol J. Bova
by Carol J. Bova
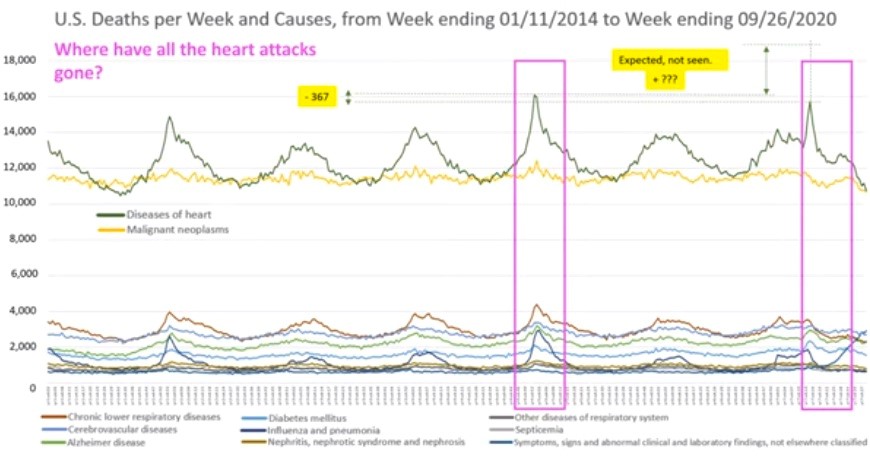
The Johns Hopkins University News-Letter published an article earlier this month asking, “Where have all the heart attacks gone?” The study questioned whether the U.S. COIVD-19 death rates are being overstated by omitting deaths usually attributed to attacks and cancer. The study was pulled four days later.
Dr. Genevieve Briand, the assistant director for the MS in Applied Economics Program at Hopkins, spoke at a webinar Nov. 11 on “COVID-19 Deaths–A Look at U.S. Data.” She meticulously detailed the facts she used and the conclusion she reached. The hour-long webinar can be viewed here.
Briand showed where and how to access the data from the Centers for Disease Control (CDC). She discussed the annual patterns of deaths in the United States and the reported number of COVID-19 deaths in relation to those annual patterns from 2014 through September, 2020.
Every year, there are recurring peaks and lows in death numbers that apply to all causes of death. She said that because of the emphasis on COVID-19, other major causes of death are being understated. She showed the percentage of total deaths by age categories and how there was no significant increase in deaths of older Americans.
The number of heart attacks and cancer, the first and second leading causes of death in the U.S., both dropped below levels expected based on previous patterns. Where all causes of death have historically spiked at the same time, for the three weeks in April when COVID-19 deaths were shown as a major spike, all other causes of death numbers dropped below the expected number in the same proportion that COVID-19 deaths increased.
Briand concluded the program with a call to the attendees to contact her if they have any ideas about why the numbers are so unusual. She urged fact checks to replicate and expand data analysis using other variables and time-series data analysis and discussed a “bottom-up approach to evidence seeking” at the state, county, township, hospital levels. She did not comment beyond explaining the methodology and showing the patterns in the CDC records since 2014, and how the COVID numbers don’t follow those patterns.
Anyone watching the presentation won’t find answers in Virginia about whether the Commonwealth’s numbers are accurate. Virginia death statistics and causes are published two or more years after the fact, the most recent is for 2017, so there is no way yet to look at changes in the total death numbers compared to prior years.
Only 6% of COVID-19 deaths have no other underlying conditions. So, even if COVID-19 is accelerating, the number of deaths that would have occurred due to heart disease or cancer, the death totals over time would not be markedly increased. Remember the September interview where Tim Powell of VDH’s Office of Epidemiology said, “If it’s on the death certificate, it’s counted. For instance, a cancer patient in hospice could count as a COVID-19 death if they also have the virus.”
So, we’re left to wonder how many COVID-19 death reports are for patients who died with COVID-19, not of COVID-19. It may be 2023 before we can find out, leaving our children falling behind with virtual classes and businesses being brought to financial ruin by COVID-19 mandates.
COVID-19 is a nasty disease, but the truth may be its worst casualty.
{kind=link}
{kind=link}
Leave a Reply
You must be logged in to post a comment.