
 by James C. Sherlock
by James C. Sherlock
We have a new General Assembly session. With that comes lots of healthcare bills.
I will not examine each one, but I have a suggestion for criteria to be applied by the Senate and House committees that do.
Ask yourselves how, if at all, each bill helps the federally designated medically underserved areas (MUAs) in Virginia.
Then ask how can any bill be a priority for funding ahead of those that do help that problem.
Then remember that providing primary care to underserved areas is proven to save a ton of Medicaid money net where it has been tried, as in Maryland, because of inpatient care avoidance.
Then ask the not-for-profit health systems that serve those areas to testify how, exactly, they can be medically underserved when that is what the health system tax exemptions are meant to prevent, and free cash flows have been extraordinary for decades.
And, finally, if you have no bills that help provide additional primary care to those areas, you aren’t doing it right.
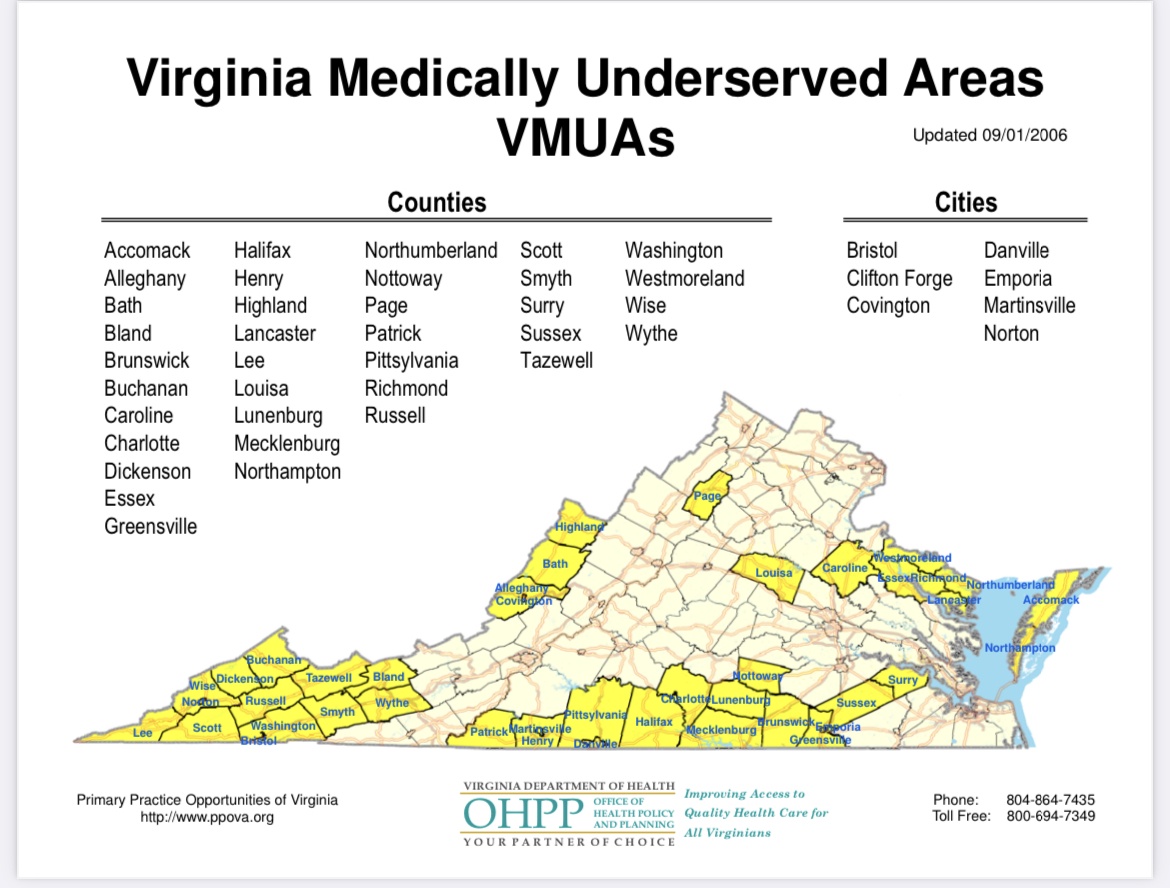
Medically Underserved Areas. MUAs as defined by the Health Resources and Services Administration (HRSA) have a shortage of primary care health services within geographic areas such as:
- a whole county;
- a group of neighboring counties;
- a group of urban census tracts; or
- a group of county or civil divisions.
I have downloaded a list of MUAs in Virginia and sorted it by need. Need, or extent of under-service, is indicated by the Index of Medical Underservice Score in the spreadsheet. The lower the number, the higher the need.
You will find some surprises there. Bipartisan surprises.
The least served areas for primary care are the Cedar Mountain and Jefferson SubDivision Service Areas in Culpeper County with an index of 42.3. Areas with a score of 50 or less (very underserved) starting with those two rural sub-divisions of Culpeper County are (rural unless designated):
- Cedar Mountain and Jefferson Subdivision Service Areas in Culpeper County 42.3
- Greensville (entire county) 42.7
- Isle of Wight (entire county 42.9 (non-rural)
- Northumberland (entire county) 43.4
- Caroline (entire county) 43.8
- Buchanan (entire county) 46.8
- Mecklenburg (entire county) 47
- Clarke (entire county) 48
- Emporia City (entire city) 48.4
- Greene County (entire county) 48.8
- Norfolk (ten census tracts) 48.8 (non-rural)
- Patrick County (entire county) 49
- Brunswick County (entire county) 49.4
- Northwest Roanoke City (seven census tracts) 50 (non-rural)
While the full list needs help, I think some bipartisan support might be found to help provide additional primary care to at least those 14 areas. In total they probably have roughly equal numbers of Democratic and Republican voters.
HEZs. I have recommended before and will again a version of Maryland’s Health Enterprise Zones (HEZs).
They have proven to save a fortune in Medicaid costs every year far in excess of the costs of the HEZs by avoided inpatient costs.
Get the not-for-profit health systems to testify. Perhaps even Virginia’s tax exempt not-for-profit healthcare systems can pitch in both to support such a bill and help directly with the problem.
In addition to Culpeper, Emporia and census tracts in Norfolk and Roanoke, census tracts in Charlottesville, Lynchburg, Hampton, Chesapeake, Virginia Beach, Newport News, Chesterfield County, Albemarle County, Fauquier County, Arlington County, and Alexandria; additional tracts in Norfolk; and all of Petersburg, Danville and Franklin City made the list.
Last I checked, all of those except Fauquier County and Danville had not-for-profit hospitals.
I did not check for this article hospital service areas in all of the medically underserved rural counties, but many of them are served by non-profit health systems as well. Committee staffers can complete the list.
The General Assembly health committees may wish to inquire of those non-profits how there could be areas underserved by primary care in their service areas. Since that is what the tax exemptions are meant to prevent. And they have been making money hand over fist for decades.
Should be an interesting session. Hope I can tune in.
Bottom line. Just a couple of thoughts.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave a Reply
You must be logged in to post a comment.