
 by Carol J. Bova
by Carol J. Bova
Governor Ralph Northam and Virginia’s public health officials say they want to “follow the science” and “follow the data” when managing the COVID-19 lockdown. Unfortunately, the data keeps changing.
Last week the Virginia Department of Health made 1,021 changes to the dataset of regional COVID-19 cases by onset date between March and October — adding 1,361 cases to the total. Forty-five percent of the dataset’s 2,258 regional entries from February through October were changed. The VDH dashboard has no footnotes explaining why the changes were made or the source of the new data.
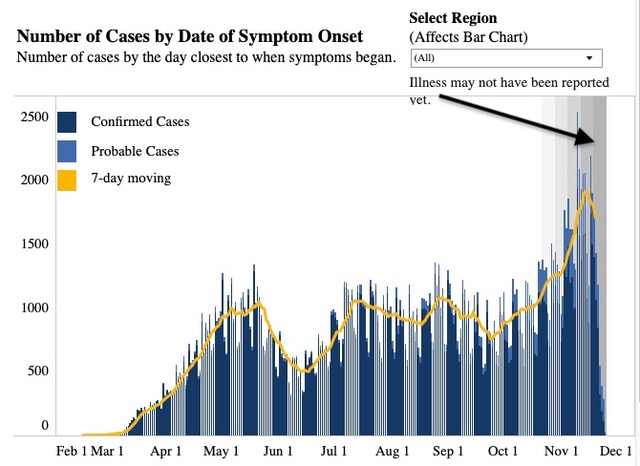
Onset date should show increasing or decreasing trends. The VDH website says, “For cases, the date of symptom onset is the closest date to when a person’s symptoms began. This measure shows increasing or decreasing trends in the number of COVID-19 cases and deaths in Virginia.” VDH also says, “Please note that data are considered preliminary and subject to change.”
Citizens must ask what validity or usefulness these changes offer one to eight months after they’ve already been considered and incorporated into the Virginia COVID-19 models and forecasts? The R0 (reproductive number) that suggests the likely spread of infections is based on recent case numbers. Were the missing numbers enough to skew the results?
Those model results and forecasts were used to evaluate the results of social behavior on virus spread and impose or relax restrictions. How long has this backfilling of months-old data been going on?
I was able to find the changes because I noticed changes in some onset dates that I had recorded. I downloaded the dataset covering dates through November 15 and so I could use that as a point of comparison with the November 23 set. Previous datasets are not available online, only the most current.
Why was months-old data entered last week? Were the changes the result of recent entries of old information to the Virginia Electronic Disease Surveillance System (VEDSS)? VDH says, “These sources include laboratory reports of COVID-19 test results, case investigation interviews conducted by the health department, monitoring of close contacts, and syndromic surveillance for coronavirus-like illness which is a system used to receive surveillance data from these various sources and report that data to CDC.”
There are questions that VDH needs to answer:
- Why would old data show up now? Who dropped the ball?
- Was contract tracing ever done on the additional cases?
- Has VDH come up with a plan to ensure timely entry of data in the future?
Some citizens might take the questioning a step further and wonder if VDH has “stockpiled” cases to guarantee a November surge to justify any actions the Governor may choose to take. Without earlier symptom onset datasets, it’s impossible to know when the backfilling started and to what degree it occurred. Without the actual data, I have to admit the thought has crossed my mind.
Carol J. Bova is a writer living in Mathews County.
Leave a Reply
You must be logged in to post a comment.