
 by Carol J. Bova
by Carol J. Bova
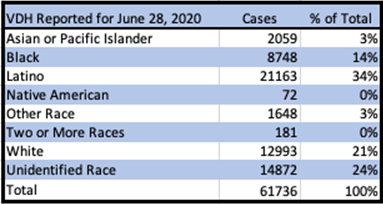
On July 27th, Bacon’s Rebellion asked the question, “Why is VDH Stockpiling Cases as Unknown Race”? The Northam administration had expressed concerns since March about the disparity of racial impacts from COVID-19. Yet 24% of confirmed cases at that time still had not been classified by race or ethnicity.
More than a month later, that percentage has barely budged. Between Aug. 1 and Sept. 5, 19% of COVID-19 cases had no racial or ethnic identifier.
On August 26, the Virginia Department of Health (VDH) discussed on its COVID-19 blog why the missing information is important and announced a new method to address the problem.
Good information on disparities in disease incidence, outcomes, and social and economic consequences, is necessary to guide and develop an appropriate response. However, efforts to study these disparities have been hampered by missing data. Almost a quarter of confirmed cases are missing race and ethnicity data. Accounting for this missing data is essential to understanding COVID-19 and to facilitate research into health disparities. Social Epidemiologists from the Office of Health Equity used imputation techniques to estimate race and ethnicity for cases missing that data.
The blog post described the process used to estimate the racial composition of COVID-19 cases that were not originally reported and showed the results. Although VDH will continue to use unimputed data on the Daily Dashboard, staff from VDH Surveillance and Investigations will post new results of the imputed numbers for research purposes as they are calculated.
But imputed data is not as good as real data.
Since August 1, labs were required to include the patient age, race, ethnicity, sex, residence zip code and county with other required info on test results, so why hasn’t the VDH Daily Dashboard improved on the number of cases with unreported race?
Who is responsible for the lack of information – are the labs failing to report as required or is VDH failing to input the data?
{kind=link}
Leave a Reply
You must be logged in to post a comment.