
The General Assembly’s key money committees gathered in their annual end-of-year financial retreats last week to talk about Medicaid. Sure, the state’s multi-billion-dollar budget delves into plenty of other areas that were mentioned, and the Amazon location announcement grabbed headlines, but the meetings were about Medicaid.
The explosive and uncontrolled growth of Medicaid is all but eliminating any new dollars for those other areas of state responsibility, and existing dollars are under pressure. There is no point in talking about anything else. The opportunity for tax reform due to windfall revenue may be short-circuited by Medicaid. If the rosy projections of new state money from Amazon come to pass, every dollar may be needed for Medicaid.
Every year the Joint Legislative Audit and Review Commission (JLARC) does this dry report about the growth in state spending. The simple bottom-line fact it has demonstrated over and over is that Medicaid is squeezing everything else out. It looks back at a ten-year period and during the ten years leading up to and including 2017, 60 percent of all General Fund growth went to for Medicaid.
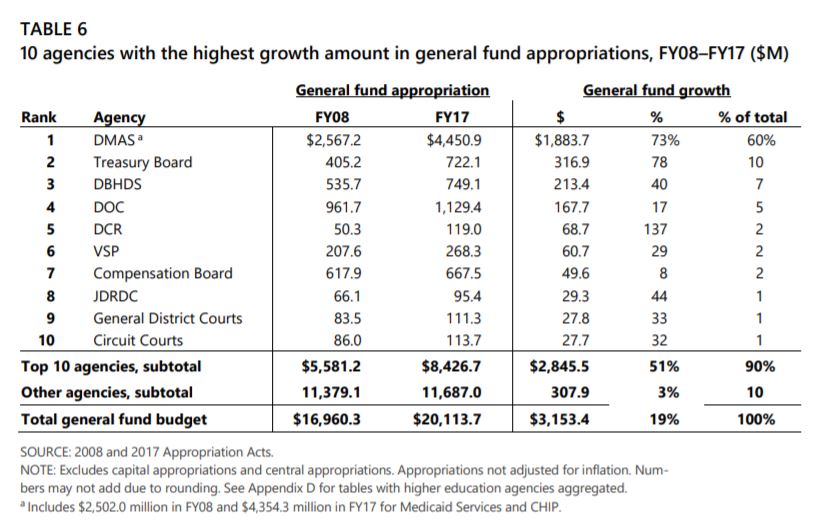
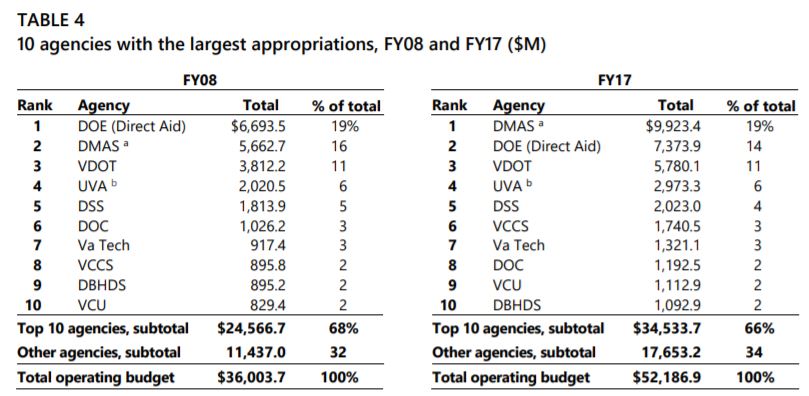
At the beginning of the period the state’s allocation to localities for public schools was the top expenditure, but it dropped down to second by Fiscal Year 2017. During that same ten-year period, from FY 2008 through 2017, the Department of Education didn’t even make the list of the ten agencies with the highest growth in General Fund dollars.
Right behind Medicaid’s 60 percent of the new money over the decade was the Treasury Board (debt payments) and the Department of Behavioral Health and Developmental Services, the other state agency providing major direct medical services to citizens. A similar chart from the 2009 report, looking at 2000-2009, had Medicaid getting 19 percent of the growth revenue, and the Department of Education 39 percent. A healthy share of growth dollars going to education may never happen again.
The figures in the JLARC report, of course, do not include the impact of the expansion of the program to an estimated 375,000 more recipients by July 2020. Nor do they include the $463 million in cost overruns announced since the budget was adopted (several months late, remember) in the existing pre-expansion program. Those will not show up in a JLARC look-back report until the 2020 report on Fiscal Year 2019.
That would be after the next election.
The state’s economy is improving and an additional $600 million or more in tax dollars are expected this year and next, the committee staffs reported, but about 75 percent of those new dollar will be needed for that overrun.
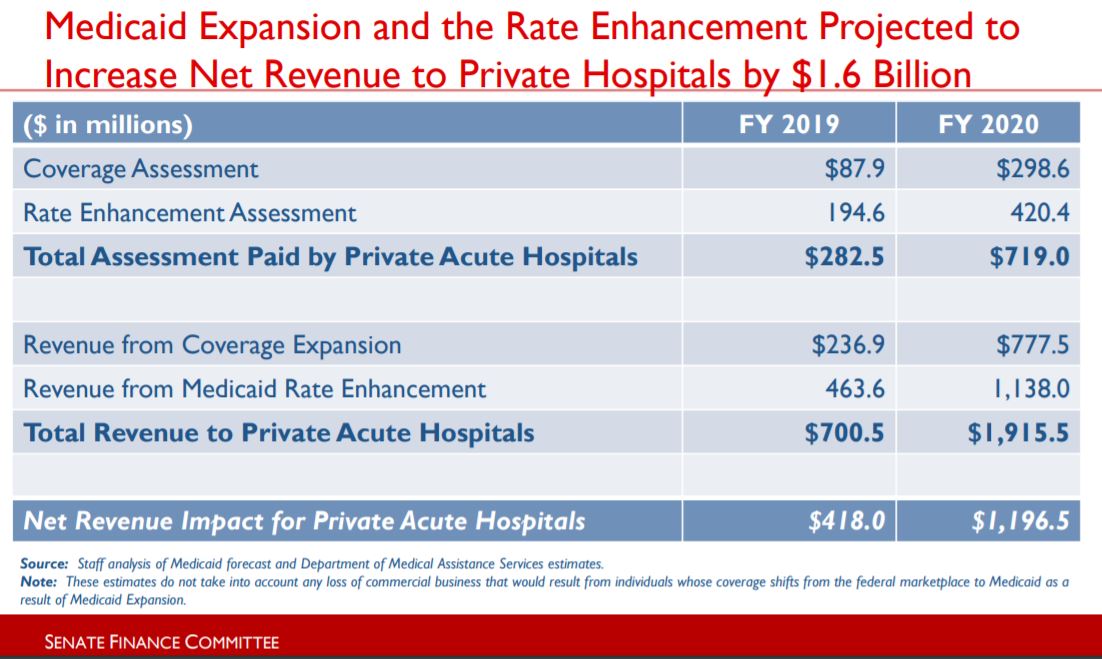
A good overview of what is going on with Medicaid is provided in a Senate Finance Committee presentation from Friday from staff analyst Mike Tweedy. The latest estimate is that the hospital provider taxes which are funding the state share of the expansion cost will collect just over $1 billion during this two-year budget cycle, which includes only 18 months of the expanded benefits.
That impressive figure was never uttered aloud during the General Assembly debate earlier this year. For that matter, the phrase “provider tax” was hardly being mentioned above a whisper. No, not that word! It’s an assessment.
Once again, as you can see in Tweedy’s chart at the start of this story, the claim (dream? hope?) is that the hospitals will just absorb that $1 billion because it is being used to draw down $2.6 billion in federal (deficit) dollars to their accounts (and of course even more federal dollars for other Medicaid providers). The hospitals will use that net $1.6 billion to treat their Medicaid patients and no additional cost comes to the rest of us.
The provider taxes on those hospitals (not all of them pay) amount to 1.7 percent of patient revenue for this year and 3.3 percent for next year, Tweedy reported. The federal rules allow states to tax Medicaid providers up to 6 percent to fund the required state match. If not the next biennium, Virginia will be there within two.
One of the very discouraging facts reported by Tweedy, and it is not news, is that Virginia may have to rebate $117 million to Medicaid because Piedmont and Catawba hospitals were not certified as psychiatric facilities. He also includes three slides (16-18) on things the state might do to improve forecasting or reign in the growth of Medicaid. None are likely to bend the curve much in the absence of a major federal push to control costs of Medicaid or of health care in general.
{kind=link}
Leave a Reply
You must be logged in to post a comment.