

by James C. Sherlock
Virginia and the nation continue to see the results of the baby bust.
I wrote yesterday of the baby cliff, the 15% decline in live births that started in the great recession of 2007-09. It continues. And it continues to drive change, much of it not good.
I have written here about such important hospital changes as:
- the closing of labor and delivery services at Virginia Beach General Hospital and elsewhere in the state; and
- the consolidation of Neo-natal ICU (NICU) services with the integration of two hospital systems into Ballad Health in Southwestern Virginia and Northeastern Tennessee.
That too is a continuing national trend.
Today’s young people of child-bearing age will find not only fewer places to deliver a child than their parents did, but also to provide specialized care if the baby needs it.
Fewer hospitals with labor and delivery services. Becker’s Hospital Review lists 13 hospitals cutting services in a recent post. Cutting services and closings posts are a regular feature of that blog.
Eight of the hospitals in that article were terminating labor and delivery services.
An example:
Hazel Crest, Ill.-based Advocate South Suburban Hospital is ending labor and delivery services on Aug. 1. The hospital cited a decline in births as the reason for the change in obstetric services, with a 40 percent decrease since 2015.
(Good news for moms — some of the birthing centers are getting nicer.)
I offer no solution, just awareness (A special shout out to Virginia’s college and university BOVs.)
Fewer Neo-natal ICU (NICU) facilities. NICUs are rarer than they used to be. Consolidating them was part of the Ballad Health fight in an area with too many opioid-addicted babies.
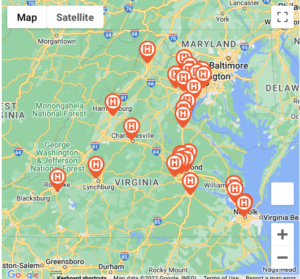
There are currently 29 NICUs in Virginia.
As you see in the adjacent map, there are no Virginia NICU facilities at all at any level west of Hampton Roads and south of Richmond, Lynchburg and Roanoke.
Some Virginians are probably closer to NICUs in adjacent states than they are to facilities in Virginia.
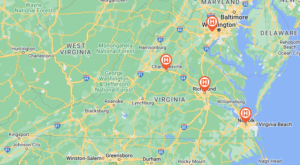
Level IV NICUs. Only four of those Virginia NICUs provide Level IV services, the highest level of care.
- Children’s Hospital of Richmond. 40 Beds
- Children’s Hospital of The King’s Daughters 64 Beds
- Inova Children’s Hospital. 108 Beds
- University of Virginia Medical Center 51 beds
Level IV is defined as a subspecialty level newborn service that:
shall provide intensive care for high-risk, critically ill neonates with complex neonatal illnesses. The subspecialty level newborn service shall provide, in-house, a full range of pediatric medical and surgical subspecialists to care for critically ill neonates.
As you see, there is no Level IV NICU facility in Virginia west of the I-64 corridor.
Babies born in these unserved areas will have to be transferred to a Level IV NICU facility if they require that level of care.
As example, below are the Level IV NICUs in North Carolina.
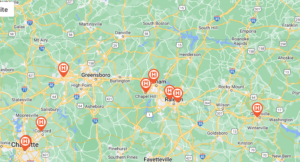
Tennessee is no help with Level IV NICUs for Virginia babies. The closest to Virginia is in Chattanooga. West Virginia? Charleston.
NICU locations are worth the expectant mother and her doctor checking if she lives in one of Virginia’s NICU deserts. OB/GYNs will certainly do that.
COPN is there for us. Virginia’s Certificate of Public Need (COPN) program, set up ostensibly to ensure that there are not “too many’ medical facilities while instead creating monopolies, cannot ensure that there are not too few.
It would be interesting to see what the COPN “need” criteria show about labor and delivery facilities and NICU.
{kind=link}
Leave a Reply
You must be logged in to post a comment.