
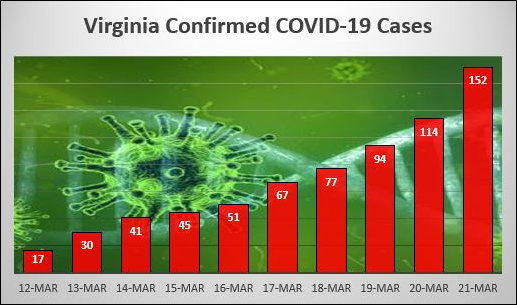
It looks like COVID-19 in Virginia is going exponential. Today’s Virginia Department of Health update of coronavirus statistics indicates that another 38 cases were confirmed yesterday, bringing the total to 152. The number of hospitalizations increased from 20 to 25. The previous one-day increase (yesterday) was only 20 cases.
To some, those might seem like small numbers. But appearances are deceiving. At the current rate of increase — doubling within the past three days — the number of confirmed cases could reach around 156,000 within a month (30 days). If the spread accelerates — say, doubling every two days — the case count would surpass five million! The latter case seems highly implausible for a variety of reasons. But even 156,000 cases would inundate hospitals and medical staff.
So far it appears than about one COVID-19 case in 10 has resulted in hospitalization. The doubling-every-three-days scenario implies that Virginia hospitals would have to cope with 15,000 to 16,000 patients, mostly toward the tail end of the 30-day period.
By my back-of-the-envelope guesstimate, Virginia hospitals should be able to handle 2,000 to 3,000 COVID-19 cases without extraordinary measures. Brace yourselves for a storm.
Leave a Reply
You must be logged in to post a comment.