
 by James A. Bacon
by James A. Bacon
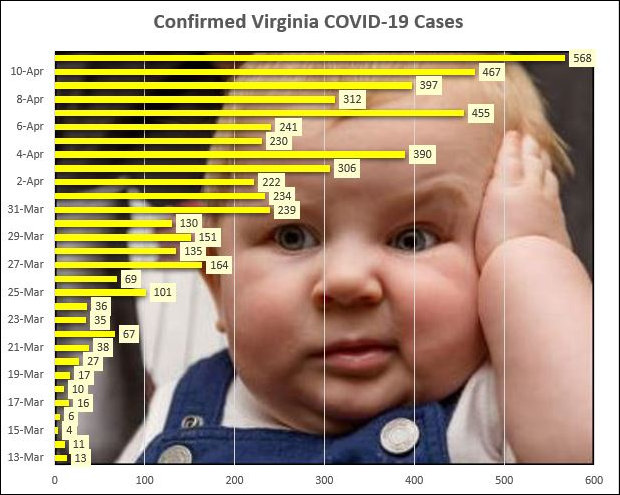
Make sense of this, if you can. Testing confirmed another 568 cases of COVID-19 in Virginia yesterday, according to Virginia Department of Health data published this morning. That was the biggest daily increase in new cases by far, bringing the total number of known cases to 5,077. Yet the number of COVID-19 cases admitted to hospitals for the virus each day hasn’t budged for eight days, and the utilization of ICUs and ventilators is down from four days ago.
Maybe this discrepancy is more apparent than real — the result of random fluctuations and reporting delays. But, then, maybe something is happening that is not fully understood. Here’s the daily data summary from VDH and the Virginia Hospital and Healthcare Association:
Total COVID-19 cases: 5,077, up 568 from the previous day
Total hospitalizations: 837, up 65 from the previous day
ICUs in use: 426, down 31
Ventilators in use: 283, up four
Total deaths: 130, up nine
Total tests: 37,999, up 2,540
% tests positive: 22.4%
Back in April 3, 66 new COVID-19 patients were admitted to hospitals. The number has bounced around between 40 and 90 in the days since, but stood at 65 yesterday. While the total number of people confirmed to have the disease has increased significantly, the number of people being hospitalized has been relatively stable. You can see the dramatic divergence here:
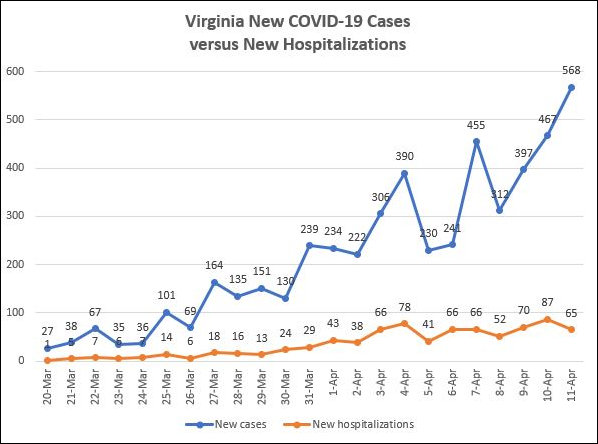
This divergence gives us some insight into why hospital capacity has yet to become a crisis beyond the shortage of personal protective equipment. For the moment at least, Virginia has an ample supply of acute care beds, ICU beds, and ventilators. That could change in a heartbeat — or a labored breath — if the virus spreads at an exponential rate and if hospitalizations start doing so as well. For whatever reason, though, the surge in new confirmed cases is not translating into a surge of hospitalized cases.
Here are John Butcher’s calculations of the doubling rate for key metrics:
Case count: 6.3 days
Hospitalizations: 6.6 days
Deaths: 4.0 days
What’s the bottom line here? If the data continue to show a divergence between COVID-19 cases and hospitalizations, it suggests that the disease is not as dangerous as we thought. Clearly, such a conclusion is highly tentative. And clearly we need to maintain social distancing to dampen the spread of the virus and ensure that hospitals aren’t overwhelmed. But perhaps we can look forward, in the not-to-distant future, to a time when we can institute baby steps to dial back the restrictions that are doing so much to damage the economy, create joblessness, and ruin peoples’ lives in ways — heightened depression, anxiety, drug and alcohol abuse, domestic abuse, suicide — that we cannot measure in real time.
Leave a Reply
You must be logged in to post a comment.