
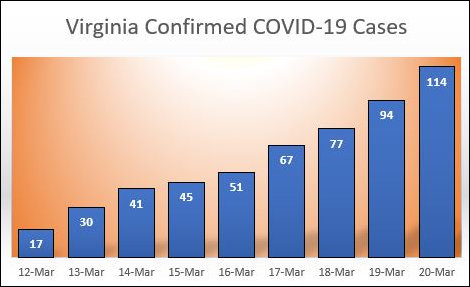
The latest count reported by the Virginia Department of Health at noon: 114 confirmed cases of the coronavirus — up 20 from the day before. The number of new cases is increasing each day. Is that evidence that the viral spread is gong exponential? Are Virginia’s social-distancing measures working?
On the other hand, consider this. Due to the shortage of testing kits, tests have been reserved for patients who seem most likely, based on their symptoms, to have a COVID-19 infection. These aren’t hypochondriacs, or random people coming off the street. For the most part, they have fevers, dry coughs and other tell-tale symptoms. even so, of 2,325 people tested to date, only 114 actually have the virus. Only 5% have tested positive. That suggests to me that community spread of the virus has yet to take off. Am I missing something?
— JAB
{kind=link}
Leave a Reply
You must be logged in to post a comment.