
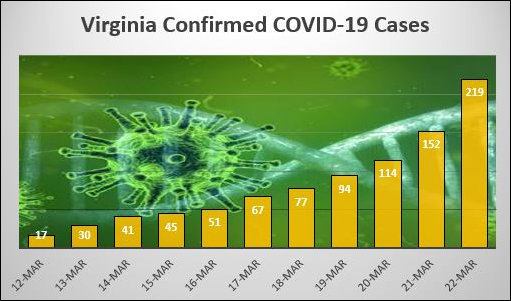
Forgive me for the mathematically nonsensical headline, but it drives home the point: Not only is COVID-19 spreading more rapidly, the rate of increase in infected patients is increasing. The Virginia Department of Health dashboard shows that 67 new cases were confirmed, and seven more coronavirus patients were admitted to hospitals. The number of fatalities rose to three.
If you’re inclined to panic, the latest data provides new fodder for your hysteria. Instead of the number of identified infections doubling every three days, as had been the case as recently as two days ago, the number has nearly doubled in just two days. The difference between doubling every three days and every two days is dramatic. If this rate of spread continues, hospitals and health care practitioners could find themselves running short of beds and staff within two to three weeks.
Governor Ralph Northam assured Virginians early in this crisis not to worry, the state had a plan. As the old military adage goes, no plan survives first contact with the enemy. In this case, no epidemic plan survives first contact with the virus. Specifically, what is being done (a) to increase the number of hospital beds, (b) increase the number of front-line health practitioners, (c) provide health practitioners the protective gear they need to avoid getting the virus themselves, and (d) create emergency capacity to hold coronavirus patients should hospitals run out of rooms?
Another question to ponder: Have the social-distancing strategies enacted here in Virginia materially slowed the spread of the disease? Without question, the measures have drastically affected the economy, but can we say that it has “flattened the curve”?
— JAB
{kind=link}
Leave a Reply
You must be logged in to post a comment.