
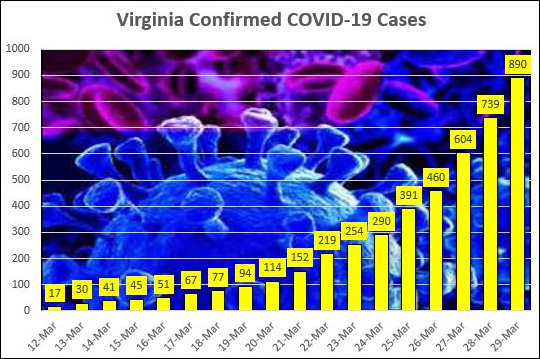
The latest numbers from the Virginia Department of Health, reflecting yesterday’s developments:
Cases: 890, up 151 from previous day.
Hospitalized: 112, up 13 from previous day.
Deaths: 22, up 5 from the previous days.
Tests: 10,609, up 1,443 from the previous day.
Here’s John Butcher’s cheerful little calculation, based on the latest data, of the “doubling time” for key Virginia metrics:
Case count: 3.14 days
Hospitalizations: 3.68 days
Deaths: 2.56 days
And then there’s this: The Institute for Health Metrics and Evaluation has forecast when the virus will start overwhelming hospital capacity in the 50 states. The Institute forecasts that Virginia will encounter “peak resource use” on May 2, 2020. At that point, 3,435 hospital beds will be needed. Virginia has more than enough beds, so there will be an acute-care “bed shortage” of zero. The problem is that Virginia will need 512 ICU beds. Only 329 will be available, creating a shortage of 183 ICU beds. Also, Virginia will have a shortage of 276 ventilators.
Deaths from the virus will peak around 30 daily. Total deaths: 1,543.
(Hat tip: Jim Loving.)
The projection assumes that social distancing measures are maintained over the next four months. Frankly, that’s not as bad as I would have expected. I wonder if the CDC will calculate the increase in alcoholism and drug overdoses, suicides, and domestic abuse murders resulting from job losses and social isolation so we can determine whether the crackdown saved lives or simply displaced lost lives from one category to another.
If these numbers are anywhere close to realistic, Virginia’s health care providers should be focusing on alleviating the shortage of ICU beds, not the overall number of hospital beds.
By the Institute’s reckoning, the shortage of acute-care and ICU beds will be far more desperate in the New York/New Jersey. Connecticut region than in Virginia. Our contagion-combating measures should not be dictated by headlines and TV broadcasts coming out of the New York area.
— JAB
Leave a Reply
You must be logged in to post a comment.