

James C. Sherlock
Elections have consequences. Democrats won fairly at the ballot box the right to pass anything they wish. I simply request that they consider the costs of legislation to their constituents, to business balance sheets, and to jobs before submitting health insurance-related bills.
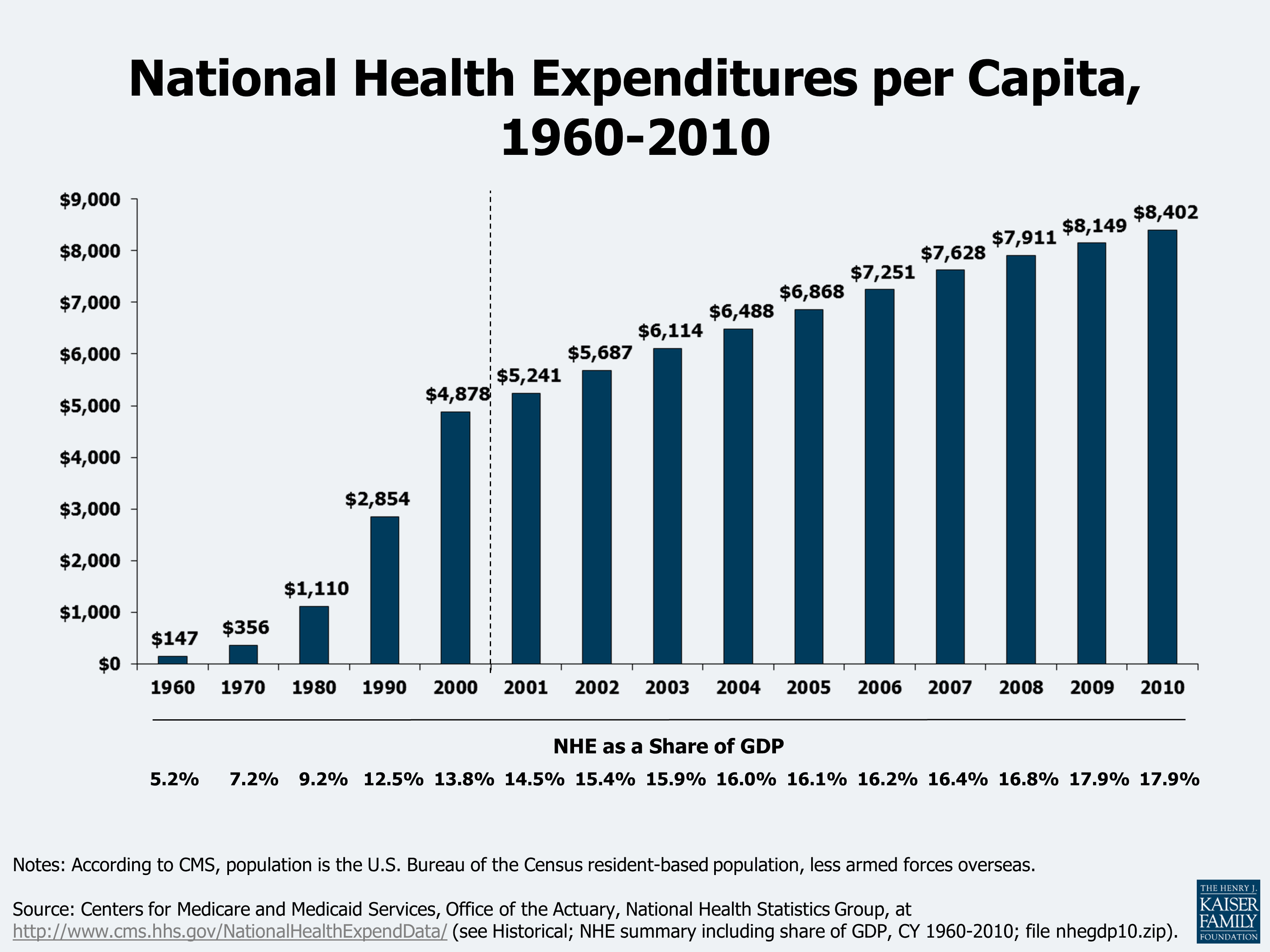
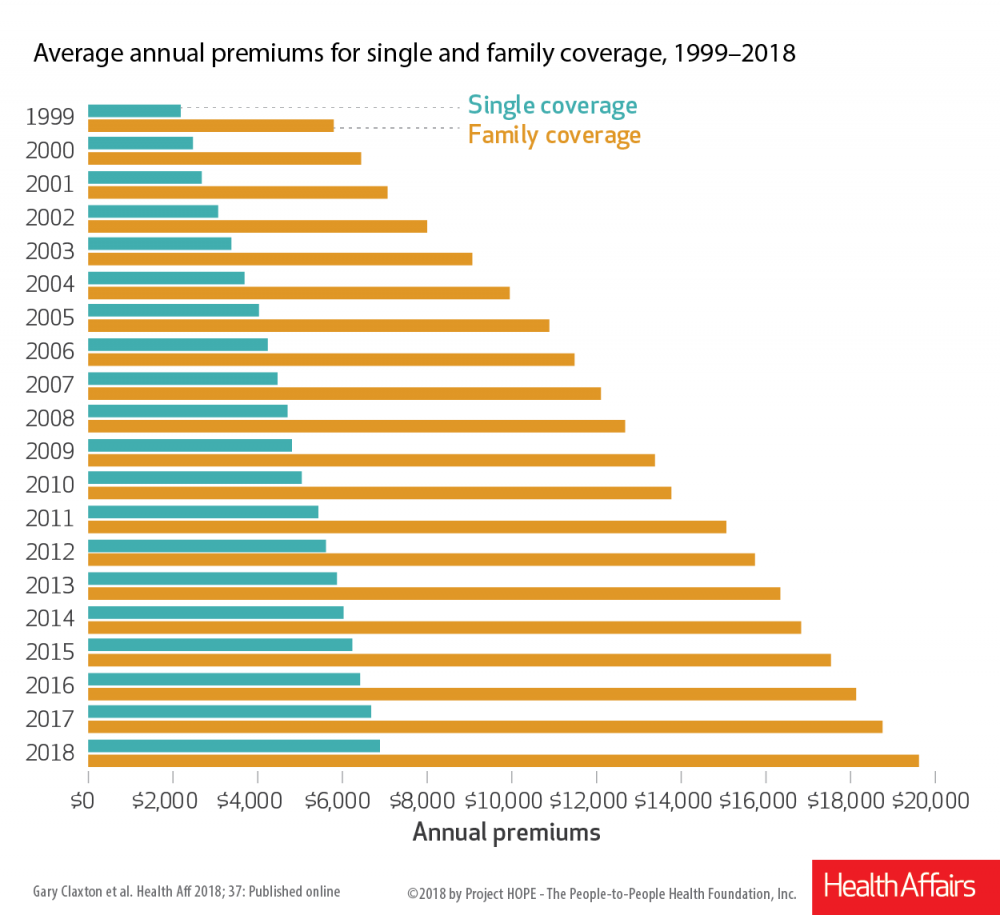
Virginians who get their health insurance both at work – which includes most of us – and get it through the Affordable Care Act website paid the highest premiums in America in 2018. The employee share of those premiums is a major and growing part of the personal budget for individuals and families statewide. The employer share comes out of employee pockets in the form of lower wages.
Bills in front of the General Assembly this year will cause those costs to skyrocket by mandating coverage of a lengthy list of additional conditions and lowering co-pays for others. Insurers will assess the costs and raise rates to cover them.
Every time the cost of health insurance goes up, businesses have to consider how to pay it. There will be layoffs. Some businesses will close. Others will look elsewhere to locate.
Eight attempt to deal with surprise billing.
Several deal with association health plans, both for and against.
I count more than 50 bills in the House and the Senate that deal with healthcare and health insurance. Most, if enacted, would push insurance costs higher. Most will directly raise the costs of health insurance by mandating additional covered conditions and procedures. These include mandated coverage for: abortion; infertility treatments; gender transition related care; autism spectrum disorder (individual and small group); six visits annually for therapy or counseling for the early detection or prevention of mental illness; fertility preservation procedures for cancer patients; zero deductible coverage for diabetes; amino acid-based elemental formula; additional mammograms at earlier ages; reproductive health (nine mandated benefits); donated human breast milk; elimination of prior authorization for drugs authorized by a psychiatrist; screening of patients for prenatal and postpartum depression; additional newborn screening; limits cost-sharing payments for insulin to $30 for a 30-day supply; zero cost sharing requirements for costs of physical therapist visits that exceed costs for a physician office visit; myoelectric, biomechanics and microprocessor-controlled prosthetic devices; hearing aids for minors; formula and enteral nutrition products for inherited metabolic disorder; and co-location of mothers with infants receiving specialized care regardless of out-of-network costs at in-network rates.
Other bills require the offering of Medicare Supplement policies to Medicare disability recipients under age 65; restrict short-term medical plans; provide new guidelines for association health plans; require hospitals to provide extended treatment procedures for emergency patients with substance abuse symptoms; require case management and peer support services for a person that has a diagnosis of substance abuse or mental health disorders; and increase staffing requirement for nursing homes.
There are 15 bills that will increase the costs of workers compensation. Many of them extend the presumption of work-related PTSD, additional named cancers, and other diseases not only to firemen and police, but to DMV officers, 911 emergency call takers, animal protection officers, police dispatchers, emergency medical technicians and correctional officers. Other bills mandate coverage of psychological injuries (really?), repetitive motion injuries and foreign injuries that are under these laws presumed to be job related. No definitive cost impact statements are required, including financial impacts to those volunteer fire departments and rescue services that pay their own workers compensation insurance bills.
Additional bills grant state licensure and qualification restrictions to special interests who have sought them. These include community health workers, diagnostic medical sonographers, musical therapists, art therapists and naturopathic doctors. That bill also gives naturopathic doctors prescription authority. Requirements for health insurance coverage for these rent seekers will follow as night follows day.
There are at least four honorable exceptions. HB 1331 (Byron-R), SB 216 (Sutterlein-R), SB 867 (Petersen-D) and HB 1094 (Miyares-R) offer paths to lower premiums. Miyares bill to multiply by an estimated factor of 7 the current number of low cost, high quality ambulatory surgical centers in Virginia can save Virginians and their health insurers, including government insurers, $500 million a year.
The members who have reintroduced bills to raise the costs of healthcare to please individual constituencies must remember that they represent all of us, not just their biggest and loudest contributors.
Note: This column has been extensively re-written since its original publication. — JAB
James C. Sherlock, a Virginia Beach resident, is a retired Navy Captain and a certified enterprise architect. As a private citizen, he has researched and written about the business of healthcare in Virginia.
{kind=link}
{kind=link}
Leave a Reply
You must be logged in to post a comment.